
Hormonal shifts in perimenopause can mimic or trigger anxiety disorders. Learn the key differences, why misdiagnosis is common, and what to ask your doctor.

Hormonal shifts in perimenopause can mimic or trigger anxiety disorders. Learn the key differences, why misdiagnosis is common, and what to ask your doctor.
You've been feeling anxious lately, really anxious. Maybe it started as a low hum of worry that you couldn't shake. Maybe it's arrived as full panic attacks, waking you up at 3 AM with a racing heart. Maybe you've already been told you have generalized anxiety disorder and handed a prescription, but something still doesn't feel right.
Here's what your doctor may not have asked: Is your anxiety new? Did it appear in your 40s, seemingly out of nowhere? Does it seem to shift with your cycle or worsen after a night of poor sleep?
If so, perimenopause may be the missing piece of your diagnosis.
A landmark 2025 study published in BMC Women's Health, analyzing Global Burden of Disease data across 204 countries, projects that anxiety disorder burden among perimenopausal women will rise by more than 40% by 2035. That's not a wellness trend. That's a clinical crisis that most of the healthcare system isn't equipped to catch. And for the millions of women currently in the middle of it, the result is often the same: anxiety treatment for what is fundamentally a hormonal problem.
This guide breaks down the science, the diagnostic gap, and the concrete differences between perimenopause-driven anxiety and a clinical anxiety disorder, so you can walk into your next appointment with better questions.
Why Perimenopause Changes Your Brain Chemistry
To understand why perimenopause so frequently produces anxiety, you have to understand what estrogen and progesterone actually do in your brain, because they do a lot more than regulate your cycle.
Estrogen and serotonin
Estrogen plays a direct role in serotonin production and receptor sensitivity. When estrogen levels are stable, your brain maintains a steady supply of serotonin, the neurotransmitter most associated with emotional stability and well-being. When estrogen drops, or more accurately, when it fluctuates erratically as it does throughout perimenopause, that stability disappears. Low serotonin is one of the primary drivers of both depression and anxiety.
Critically, it's not just the level of estrogen that matters. Research shows that the rate of change has its own neurological impact. A rapid hormonal shift can overwhelm the brain's regulatory systems even when hormone levels technically fall within a "normal" lab range, which is one reason so many women with perimenopausal anxiety are told their bloodwork looks fine.
Progesterone, GABA, and your brain's natural anxiety relief
Progesterone is often overlooked in conversations about anxiety, but its role is central. Progesterone produces a metabolite called allopregnanolone (ALLO), which directly activates GABA-A receptors in the brain. GABA is the nervous system's primary inhibitory neurotransmitter, the biological equivalent of a braking system for anxiety. It's the same receptor system targeted by benzodiazepines like Xanax or Valium.
As progesterone falls during perimenopause, ALLO levels fall with it. That braking system weakens. The result is a nervous system that's more easily excitable, more reactive to stress, and less able to return to calm, not because of a psychological disorder, but because of a specific hormonal mechanism.
This is why many women describe perimenopausal anxiety as feeling different from stress they've experienced before: more physical, more sudden, harder to talk themselves out of.
Why the Diagnostic Tools Are Stacked Against You
Here's a structural problem that rarely gets discussed openly: the standard screening tools your doctor uses to assess your mental health were not designed to account for hormonal drivers.
The PHQ-8, one of the most commonly used depression screens, has 8 indicators. Let's look at how many of them perimenopause can cause directly:
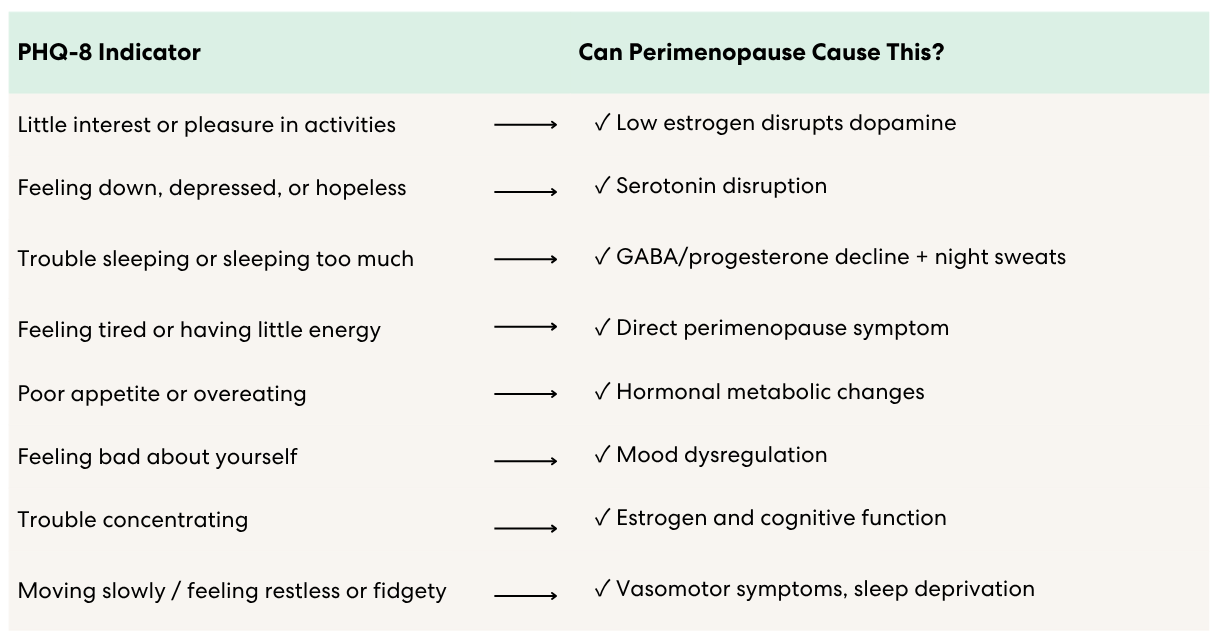
Seven out of eight. A clinician running through this checklist without asking a single question about your menstrual history, your cycle regularity, hot flashes, or the timeline of your symptoms is very likely to arrive at a depression or anxiety diagnosis, and miss the hormonal driver entirely.
The GAD-7, the standard tool for screening generalized anxiety disorder, has the same limitation. It measures the presence and severity of anxiety symptoms. It cannot distinguish between anxiety rooted in a clinical disorder and anxiety rooted in hormonal fluctuation. That distinction requires a conversation about your hormonal context, one that too rarely happens.
Perimenopause Anxiety vs. GAD: Key Differences
Both can be real. Both can be serious. And both can exist in the same person at the same time. But understanding the differences is essential for getting the right treatment.
.png)
A note on overlap: Many women have both. Perimenopause can trigger a first episode of GAD in women who have a biological predisposition to anxiety. The goal isn't to prove it's one or the other, it's to make sure the hormonal component isn't being missed.
The Study of Women's Health Across the Nation (SWAN), one of the most comprehensive longitudinal studies of women through the menopausal transition, found that women with low baseline anxiety were significantly more likely to develop high anxiety during perimenopause, with odds ratios of 1.56 to 1.61, independent of other life stressors, financial strain, or vasomotor symptoms. In other words, perimenopause creates new anxiety risk even in women who've never struggled with it before.
Signs Your Anxiety May Be Hormonally Driven
Not every anxiety symptom in your 40s is perimenopause. But the following patterns point strongly toward a hormonal driver:
- Your anxiety appeared for the first time in your 40s (or late 30s), no prior anxiety history
- It worsens around your period, or in the days after a night of hot flashes and disrupted sleep
- You're also experiencing irregular cycles, spotting between periods, brain fog, joint pain, or bloating
- You have significant bloating or digestive changes alongside mood shifts, gut-hormone connections are real
- Standard anxiety treatments haven't worked the way you expected
- Your doctor hasn't asked about your menstrual history, cycle changes, or whether you might be in perimenopause
- Your bloodwork came back "normal" but you still feel terrible
The last point is important. Hormone levels fluctuate significantly during perimenopause, sometimes hour to hour. A single blood draw is a snapshot, not a pattern. Normal FSH on a Tuesday doesn't mean your estrogen didn't crater on Thursday and send your nervous system into overdrive.
What to Do Next
1. Track your symptoms against your cycle
Keep a simple log, dates, symptoms, severity, sleep quality, cycle day if your periods are still regular. Bring it to your appointment. A written, time-stamped pattern is much harder to dismiss than a verbal description.
2. Name perimenopause explicitly
Don't wait for your doctor to raise it. Say directly: "I think perimenopause may be contributing to my anxiety, and I'd like to explore that." Studies show only a minority of clinicians initiate this conversation. You may have to start it.
3. Ask for a hormonal workup, and ask the right questions
Request FSH, estradiol (E2), and if possible AMH (anti-Müllerian hormone, which tracks ovarian reserve). Ask for the test to be repeated across your cycle rather than relying on a single draw. And know that results can fall in the "normal" range while perimenopause is still driving your symptoms.
4. Ask about hormone therapy as part of the conversation
If your anxiety is tied to hormonal fluctuation, addressing it at the hormonal level may be part of the solution, not instead of mental health treatment, but alongside it. HRT isn't right for everyone, but it should be on the table for women whose anxiety is clearly cyclical and correlated with hormonal shifts.
5. Consider a specialist
If your primary care physician or OB/GYN isn't familiar with perimenopausal mental health, ask for a referral to a certified menopause practitioner (NAMS-certified), a reproductive psychiatrist, or an integrative women's health specialist. This field exists. You deserve someone who has trained in it.
6. Support your nervous system while you work on the root cause
Some supplements may help stabilize mood during perimenopause, and evidence-based approaches like CBT remain effective for anxiety regardless of cause. Both can be valuable bridges while you pursue hormonal evaluation and treatment.
Frequently Asked Questions
Can perimenopause cause panic attacks?
Yes. The same GABA and serotonin disruptions that produce generalized anxiety can also trigger panic attacks, sudden, intense episodes of physical fear with a racing heart, shortness of breath, or a sense of dread. If you're experiencing panic attacks for the first time in your 40s, perimenopause is a clinically plausible explanation that warrants investigation.
How do I know if my anxiety is hormonal?
The clearest signals are: new onset in your 40s with no prior history, cyclical timing (worse around your period or after night sweats), and co-occurrence with other perimenopause symptoms like brain fog, irregular periods, or sleep disruption. Tracking symptoms over 6–8 weeks against your cycle will give you, and your doctor, meaningful data.
Will HRT help my anxiety?
For women whose anxiety is driven by hormonal fluctuation, hormone therapy can be significantly effective, particularly for estrogen-related mood instability. The evidence is strongest for women in early perimenopause. It's less likely to resolve a primary anxiety disorder on its own, which is why accurate diagnosis matters. Read more about how to know if your HRT dose is working.
My doctor says my hormones are normal. Can I still be in perimenopause?
Yes. Hormone levels fluctuate dramatically during perimenopause and a single blood test often misses the pattern. It's entirely possible to have a normal FSH result while experiencing significant perimenopausal symptoms. Symptom tracking alongside hormone testing gives a more complete picture.
What's the difference between perimenopause anxiety and PMDD?
PMDD (premenstrual dysphoric disorder) involves severe mood symptoms in the 1–2 weeks before your period, resolving when your period starts. Perimenopausal anxiety can be more continuous and less predictably tied to the luteal phase, particularly as cycles become irregular. Some women who previously had PMDD find that symptoms intensify and shift during perimenopause as hormone fluctuations become less predictable.
About the author
Sources
- Zhang Y, Hu TT, Cheng YR, Zhang ZF, Su J. Global, regional, and national burden of anxiety disorders during the perimenopause (1990–2021) and projections to 2035. BMC Women's Health. 2025;25(1):11. https://doi.org/10.1186/s12905-025-03547-z
- Bromberger JT, Kravitz HM, Chang YF, et al. Does risk for anxiety increase during the menopausal transition? Study of Women's Health Across the Nation. Menopause. 2013. PMID: 23615639.
- Hormonal Balance and the Female Brain: A Review. FACTS About Fertility. https://www.factsaboutfertility.org/hormonal-balance-and-the-female-brain-a-review/
- Lang XL et al. From physiology to psychology: An integrative review of menopausal syndrome. World Journal of Psychiatry. 2025;15(11):108713. https://doi.org/10.5498/wjp.v15.i11.108713
- Estrogen and anxiety: connection, causes, and treatments. ScienceInsights. 2025. https://scienceinsights.org/what-is-the-connection-between-estrogen-and-anxiety/
- Anxiety Disorders Among Women: A Female Lifespan Approach. Focus (American Psychiatric Association Publishing). https://psychiatryonline.org/doi/10.1176/appi.focus.20160042
- Gibson CJ et al. A Systematic Review of Anxiety and Depressive Symptoms Among Women Experiencing Vasomotor Symptoms Across Reproductive Stages in the US. International Journal of Women's Health. 2025;17:537–552. https://doi.org/10.2147/IJWH.S491640
About the Oova Blog:
Our content is developed with a commitment to high editorial standards and reliability. We prioritize referencing reputable sources and sharing where our insights come from. The Oova Blog is intended for informational purposes only and is never a substitute for professional medical advice. Always consult a healthcare provider before making any health decisions.



