
Mood crashes before your period. Anxiety that appears out of nowhere. Rage that feels disproportionate and then disappears. It could be PMDD. It could be perimenopause. Or it could be both, which is why so many women in their late 30s and 40s spend years cycling through the wrong diagnosis. Here's how to tell the difference, what the hormone data actually shows, and what to bring to your next appointment.

Mood crashes before your period. Anxiety that appears out of nowhere. Rage that feels disproportionate and then disappears. It could be PMDD. It could be perimenopause. Or it could be both, which is why so many women in their late 30s and 40s spend years cycling through the wrong diagnosis. Here's how to tell the difference, what the hormone data actually shows, and what to bring to your next appointment.
You know the feeling. A week before your period, something shifts. The anxiety that was manageable becomes overwhelming. Small frustrations become unbearable. You feel like a completely different person, and then, almost as suddenly as it arrived, it lifts the moment your period starts.
For years, you called it bad PMS. Maybe a doctor called it PMDD. You adjusted your schedule, warned people around you, and learned to wait it out.
But now you're in your early 40s and something has changed. The mood crashes are worse. They're happening at different times. Some months the pattern you knew doesn't show up at all, replaced by something more constant, more unpredictable, harder to explain.
Is it still PMDD? Is it perimenopause? Is it both?
This is one of the most common, and most consequential, diagnostic confusions in women's health. And it matters, because PMDD and perimenopause share almost identical surface symptoms but have different hormonal drivers, different trajectories, and different treatment approaches. Getting the diagnosis wrong doesn't just delay relief. It can mean years of treating the wrong thing.
The single clearest distinction between the two: PMDD follows the cycle. Perimenopause disrupts the cycle.
Everything else flows from that.
Why This Gets Confused So Often
PMDD (Premenstrual Dysphoric Disorder) and perimenopause both involve estrogen and progesterone. Both affect mood, sleep, anxiety, and cognitive function. Both are cyclical, or appear to be. And both tend to be dismissed, minimized, or misdiagnosed as generalized anxiety or depression.
The overlap is real. But the mechanism behind the symptoms is different, and that difference changes everything about what helps.
The place to start is understanding what each condition actually is, not just what it feels like.
What PMDD Actually Is
PMDD is not a mood disorder in the traditional sense. It's a sensitivity disorder, specifically, an abnormal neurological response to normal hormonal fluctuations.
Women with PMDD have estrogen and progesterone levels that are, in most cases, within normal range. What's different is how their brain responds to the drop in progesterone that happens in the late luteal phase, the week or two before menstruation. That progesterone drop triggers a cascade that affects serotonin, GABA, and other neurotransmitters, producing the severe mood symptoms that define the condition: dysphoria, anxiety, irritability, and in some cases, suicidal ideation.
The hallmark of PMDD is its predictability and its complete resolution. Symptoms appear in a tight window, typically the 5 to 7 days before menstruation, and disappear within 1 to 2 days of bleeding starting. If you've been tracking your cycle and your worst days are reliably in that late luteal window, and you reliably feel like yourself again once your period arrives, that pattern is strongly suggestive of PMDD.
Low progesterone plays a role in this picture, but the mechanism is more precise than progesterone deficiency alone: when progesterone falls in the luteal phase, it takes with it a neurosteroid called allopregnanolone that acts on GABA receptors in the brain, the same receptors targeted by anti-anxiety medications. In women with PMDD, the brain's sensitivity to this normal progesterone withdrawal is abnormally amplified. The hormone levels themselves may be within range. The neurological response to their fluctuation is not.
What Perimenopause Actually Is
Perimenopause is the hormonal transition that precedes menopause, typically beginning in the early-to-mid 40s though it can start earlier. Unlike PMDD, where hormone levels are often within normal range, perimenopause is defined by actual hormonal change, specifically, the increasing variability and eventual decline of estrogen and progesterone as ovarian function shifts.
The key word is variability. Perimenopausal hormone fluctuations are not predictable. Estrogen can spike dramatically and then crash within the same cycle. Progesterone production becomes less consistent. Cycles that were once regular may shorten, lengthen, or become unpredictable. Mood swings, brain fog, insomnia, and anxiety can appear at any point in the cycle, not just in the luteal phase, because the hormonal fluctuations driving them are no longer on a predictable schedule.
This is the core clinical distinction: PMDD follows the cycle. Perimenopause disrupts the cycle itself.
The Symptom Overlap, and Where They Diverge
Both conditions can cause:
Severe mood shifts, including irritability, rage, sadness, and emotional dysregulation. Sleep disruption, difficulty falling asleep, staying asleep, or waking early. Anxiety that feels disproportionate to circumstances. Brain fog and difficulty concentrating. Physical symptoms like bloating, breast tenderness, and headaches.
The symptoms look identical on paper. In practice, the difference is in the timing and the pattern.
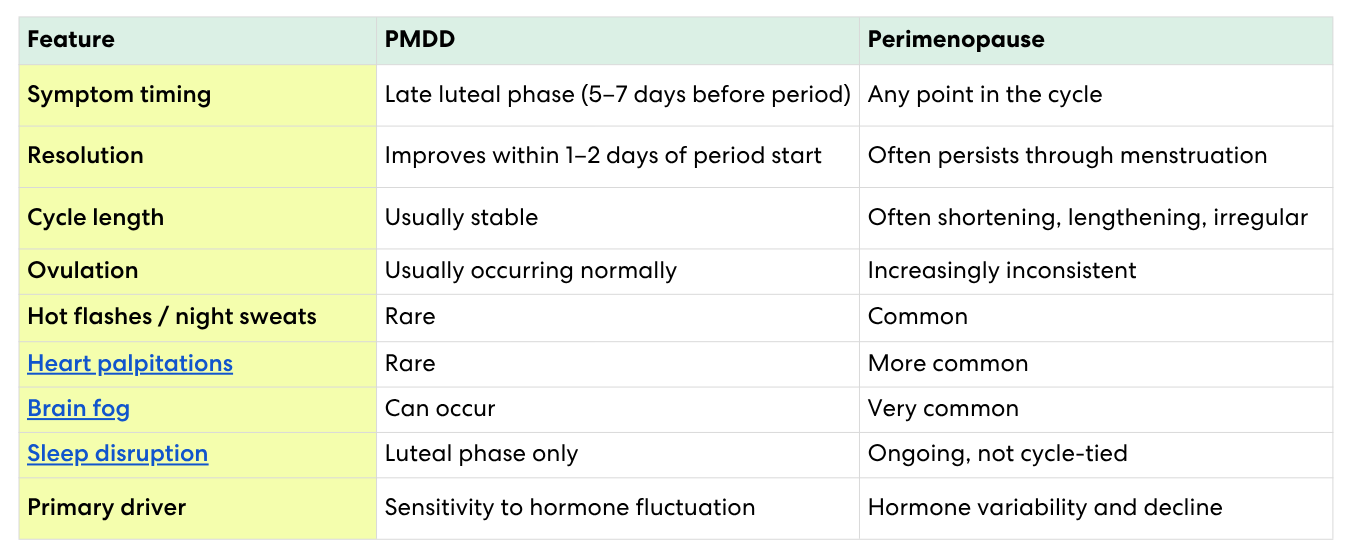
In PMDD: Symptoms cluster reliably in the 5–7 days before menstruation. They resolve within 1–2 days of the period starting. The follicular phase, the first half of the cycle, is typically symptom-free. The cycle itself remains regular.
In perimenopause: Symptoms can occur at any phase of the cycle, including mid-cycle or even in what used to be the "good week." They may not resolve when menstruation begins. The cycle itself begins to change, shorter, longer, heavier, lighter, or skipped entirely. Spotting between periods may appear. Heart palpitations, hot flashes, and night sweats, which are not features of PMDD, may emerge.
One of the most recognizable signs of this shift: many women with PMDD describe having one bad week per cycle, predictable, contained, survivable. Women transitioning into perimenopause often describe something quite different: the disappearance of the good week entirely. Not one bad week. No reliable good week. Just a baseline that used to exist and now doesn't.
That loss of the predictable symptom-free window is one of the clearest clinical signals that perimenopause has entered the picture, regardless of whether PMDD was present before.
Can PMDD Start in Your 40s?
This is one of the most common questions in perimenopause communities, and one of the most important to answer carefully.
True new-onset PMDD beginning for the first time in your 40s is less common than it appears. What's far more likely in most cases is one of three things:
First, mild PMDD that was present for years but manageable is now being amplified by perimenopause's increasing hormone variability. The underlying sensitivity was always there. The worsening hormonal backdrop is making it more visible and more severe.
Second, what feels like new PMDD is actually perimenopause-driven hormone volatility being misread as a luteal-phase condition. Estrogen that spikes and crashes in the follicular phase, for example, can cause symptoms that feel like they're following a cycle even when they're not tied to the luteal phase at all.
Third, a small subset of women do experience genuine late-onset PMDD, typically associated with a significant hormonal trigger like stopping hormonal contraception, postpartum hormone shifts, or the hormonal volatility of early perimenopause itself.
In all three cases, the distinguishing factor is the same: symptom timing relative to cycle phase, tracked across multiple cycles, with hormone data to confirm what the pattern actually is. A woman who thinks she's developing PMDD at 43 may be, but she's more likely entering perimenopause, and the treatment path is different enough that the distinction matters enormously.
Here's what makes this clinically difficult, and what no one tends to explain clearly: PMDD and perimenopause are not mutually exclusive. In fact, women who had PMDD earlier in their reproductive years often experience a significant worsening of their symptoms as they enter perimenopause, because the hormonal variability of the transition amplifies the neurological sensitivity that drove their PMDD in the first place.
This is sometimes called "perimenopausal PMDD" or "PMDD overlap," and it presents as PMDD symptoms that are becoming more severe, less predictable, or longer-lasting than before, as if the condition is expanding beyond its original tight luteal-phase window.
For these women, the trajectory of change is the diagnostic signal. If PMDD symptoms that were manageable for years are suddenly worse, starting earlier in the cycle, lasting longer, or no longer fully resolving with menstruation, that evolution is likely being driven by the hormonal shifts of perimenopause layered on top of pre-existing PMDD sensitivity.
Why Standard Testing Often Fails Both
A single FSH or estradiol blood test is commonly used to evaluate whether a woman is in perimenopause. But as we discuss in our guide to hormone testing, a one-time snapshot has significant limitations in the early transition. Perimenopause is characterized by erratic fluctuation, not consistent elevation or decline. An FSH drawn on the wrong day of a variable cycle can look entirely normal even when the transition is well underway.
The same problem applies to PMDD evaluation. Standard workups don't measure progesterone or allopregnanolone dynamics across the luteal phase, they look for abnormal hormone levels. But PMDD isn't caused by abnormal levels. It's caused by a normal pattern experienced abnormally. A blood panel that comes back "normal" is not a refutation of PMDD. It's a reflection of what single-point testing can and cannot see.
This is why so many women spend years without a clear answer: not because the answer doesn't exist in their hormone data, but because the measurement was never taken at the right resolution or across enough time.
Two Women, Identical Symptoms, Different Diagnoses
Consider two women, both 42, both experiencing severe mood crashes, anxiety, and sleep disruption.
The first tracks her symptoms and notices they arrive like clockwork on day 22 of her 28-day cycle and completely resolve on day 2 of her period. Her cycles are regular, 27–29 days. She has no symptoms mid-cycle. She describes herself as "a different person for 6 days and then completely fine." That pattern, luteal onset, full resolution, cycle regularity, is PMDD.
The second notices that her mood crashes used to be predictable but now seem to happen at different times each month. Last month it was mid-cycle. This month it started on day 18 and still hadn't resolved when her period arrived. Her cycles have shortened from 28 days to 24 days. She's also started waking at 3am and had two episodes of heart palpitations. That pattern, unpredictable onset, incomplete resolution, cycle changes, new physical symptoms, is perimenopause.
Both women are suffering. Both deserve answers. The path to those answers runs through the pattern in their hormone data, not through a single checklist appointment.
Why Symptom Tracking Alone Often Isn't Enough
Symptom journaling is a useful starting point, but it has a ceiling. Two women can have nearly identical symptom logs and completely different hormone patterns driving them.
One may have classic PMDD: symptoms tightly linked to progesterone withdrawal in the luteal phase, a clean hormone curve that follows the cycle precisely, a follicular phase that's entirely symptom-free.
Another may have estrogen volatility characteristic of early perimenopause: symptoms appearing mid-cycle when estrogen spikes and crashes, progesterone rising inconsistently, mood disruption that doesn't map onto any predictable cycle phase at all.
Both women might write in their journals: "terrible anxiety, couldn't sleep, felt like a different person." The symptom description is identical. The hormone pattern tells a completely different story, and points toward a completely different intervention.
This is the gap between tracking how you feel and understanding why. Symptom logs capture the experience. Hormone data captures the mechanism. For a condition where the mechanism determines the treatment, one without the other leaves the most important question unanswered.
What the Hormone Pattern Actually Shows
The clearest way to distinguish PMDD from perimenopause, and to identify the overlap, is to track estrogen, progesterone, and LH across multiple complete cycles.
In PMDD without perimenopause, you'll typically see a recognizable hormonal pattern: estrogen and LH rise and fall on schedule, progesterone rises post-ovulation, and symptoms correlate tightly with the late progesterone decline. The pattern is consistent cycle to cycle.
In perimenopause, the pattern is disrupted. Estrogen may spike unpredictably. Progesterone production becomes less robust, sometimes failing to rise meaningfully after a cycle in which ovulation was incomplete or absent. LH levels may begin to trend higher. Cycle length begins to vary. When you can see these hormone patterns across multiple cycles rather than estimating from a single blood draw, the clinical picture becomes far more legible.
In overlap cases, you'll often see a recognizable PMDD-pattern progesterone sensitivity amplified by increasing estrogen volatility, the late luteal drop is happening against a backdrop of hormones that are no longer stable the rest of the month.
Understanding what progesterone is actually doing across your cycle, not just what a single number says, is what transforms this from a diagnostic guess into a clinical answer.
What to Bring to Your Provider
Whether you suspect PMDD, perimenopause, or both, the most valuable thing you can bring to a clinical conversation is documented pattern data, not a description of symptoms from memory.
Specifically, it helps to have:
A symptom log with dates, mapped against your cycle phase, covering at least two to three cycles. Note when symptoms start, when they peak, whether they resolve with menstruation, and whether there's a symptom-free window in the first half of your cycle.
Hormone tracking data showing estrogen, progesterone, and LH across a full cycle or more, ideally including both the follicular and luteal phases. A pattern that shows progesterone dynamics across the luteal phase is far more informative than a single mid-cycle blood draw.
A record of cycle changes: length, flow, any new symptoms like spotting, palpitations, or night sweats that suggest perimenopause rather than PMDD alone.
This data changes the conversation. Instead of describing how you feel and waiting to be believed, you're bringing a pattern that speaks for itself.
What to Expect From Treatment
Treatment differs meaningfully depending on which condition is driving symptoms, which is another reason getting the diagnosis right matters.
For PMDD, first-line treatments typically include SSRIs (used continuously or luteal-phase only), hormonal interventions like continuous low-dose oral contraceptives or progesterone supplementation, and lifestyle approaches targeting the luteal phase specifically.
For perimenopause, the evidence increasingly supports hormone therapy, particularly estradiol, as the most effective intervention for mood, sleep, and cognitive symptoms. If PMDD sensitivity is also present, progesterone type and timing within HRT matters significantly: oral micronized progesterone appears to have more favorable neurological effects than synthetic progestins for women with PMDD-like sensitivity.
For overlap cases, treatment is more nuanced, and more dependent on understanding the individual hormone pattern than on applying a standard protocol. The women most likely to get good outcomes from treatment are the ones whose providers can see not just what hormones to prescribe, but what the pattern shows about how those hormones are being received.
Oova tracks estrogen (E3G), progesterone (PdG), and LH daily, giving you the full hormone pattern across your cycle, not just a snapshot. Whether you're trying to understand PMDD, perimenopause, or the overlap, the pattern is where the answer lives. 99% correlated to blood testing. HSA/FSA eligible.
Stop guessing which one it is. See your hormone pattern across a full cycle. →
About the author
Sources
- Hantsoo L, Epperson CN. "Premenstrual Dysphoric Disorder: Epidemiology and Treatment." Current Psychiatry Reports. 2015;17(11):87.
- Bäckström T, et al. "The role of hormones and hormonal treatments in premenstrual syndrome." CNS Drugs. 2003;17(5):325–342.
- Freeman EW, et al. "Core symptoms that discriminate premenstrual syndrome." Journal of Women's Health & Gender-Based Medicine. 2000;9(5):553–558.
- Bromberger JT, et al. "Major depression during and after the menopausal transition: SWAN Mental Health Study." Psychological Medicine. 2011;41(9):1879–1888.
- Soares CN. "Depression and Menopause: Current Knowledge and Clinical Recommendations for a Critical Window." Psychiatric Clinics of North America. 2017;40(2):239–254.
- Rapkin AJ, Lewis EI. "Treatment of premenstrual dysphoric disorder." Women's Health. 2013;9(6):537–556.
- Prior JC. "Progesterone for Symptomatic Perimenopause Treatment." Facts Views Vis Obgyn. 2011;3(2):109–120.
About the Oova Blog:
Our content is developed with a commitment to high editorial standards and reliability. We prioritize referencing reputable sources and sharing where our insights come from. The Oova Blog is intended for informational purposes only and is never a substitute for professional medical advice. Always consult a healthcare provider before making any health decisions.



