
Starting HRT and wondering when you'll actually feel better? Different symptoms respond at different times, and knowing the real timeline can stop you from giving up too early or assuming something is wrong. This is your week-by-week guide to what HRT is doing in your body, from day one through month three and beyond.

Starting HRT and wondering when you'll actually feel better? Different symptoms respond at different times, and knowing the real timeline can stop you from giving up too early or assuming something is wrong. This is your week-by-week guide to what HRT is doing in your body, from day one through month three and beyond.
One of the most common questions asked the week after starting HRT is some version of this: When is this supposed to kick in?
It's a reasonable question. You've done the research, you've had the appointment, you've filled the prescription. But the first days can feel anticlimactic, or in some cases, temporarily worse. Hot flashes still happening. Sleep still disrupted. Mood still all over the place.
What most people aren't told upfront is that HRT doesn't work like a light switch. Different symptoms respond on different timelines, driven by how your body reuptakes estradiol at the tissue level, how long it takes for certain systems to recalibrate, and whether your starting dose is actually right for you.
This guide lays out what the research and clinical experience tell us about when to expect relief, symptom by symptom, week by week.
A note before we start: This timeline reflects general patterns for systemic HRT. Your specific form, pill, patch, gel, or cream, and your individual hormone baseline will affect your experience. If your timeline looks meaningfully different from what's described here, that's worth discussing with your provider, not waiting out silently.
Before Week 1: What's Happening in Your Body Before You Feel Anything
In the first few days after starting HRT, your body is absorbing estradiol and beginning the process of binding it to estrogen receptors distributed throughout multiple organ systems, your brain, cardiovascular system, gut, bone, and urogenital tract among them.
This receptor re-sensitization doesn't produce immediate symptomatic change. You're essentially restocking a depleted system, and the downstream effects take time to express. Think of it less like flipping a switch and more like slowly refilling a reservoir.
Some women notice a mild initial increase in breast tenderness or bloating in this first window. This is normal, estradiol is beginning to act on breast and uterine tissue, and it typically resolves within the first few weeks as your body adjusts.
Weeks 1–2: The First Signals
What you may notice:
- Modest reduction in hot flash intensity or frequency in some women
- Possible initial breast tenderness, bloating, or mild nausea (particularly with oral estradiol)
- Improved sense of wellbeing reported by some women even before physical symptoms fully change, likely due to estrogen's early effects on serotonin activity in the brain
- Sleep may begin to shift slightly, though this is rarely dramatic yet
What's still unchanged for most people:
- Night sweats may persist
- Vaginal dryness is unlikely to show improvement yet
- Brain fog, concentration, and memory are typically unchanged
- Mood stabilization is usually incomplete
The first two weeks are essentially a calibration period. If you feel a subtle shift in mood or energy, that's real, estradiol has measurable effects on neurotransmitter activity relatively quickly. But if you don't notice much yet, that's also normal. You're not in the window where most symptoms resolve.
Weeks 2–4: Vasomotor Symptoms Begin to Improve
Hot flashes and night sweats are typically the first symptoms to respond to HRT, and most women begin noticing meaningful improvement somewhere in this window, though full relief often takes longer.
Clinical trials consistently show that hot flash frequency and severity begin declining within 2–4 weeks of starting estrogen therapy. A landmark review of randomized controlled trials found that estrogen reduced hot flash frequency by approximately 75% compared to placebo, with benefit beginning to accumulate in this early window and continuing to build over the subsequent months.
What this looks like in practice: hot flashes may become less intense before they become less frequent. Or you may notice fewer nighttime episodes before daytime ones settle. The pattern varies, but direction of travel should be toward improvement.
Sleep often starts improving in this window for women whose primary sleep disruptor was night sweats, because fewer overnight hot flashes means fewer arousals. But if your sleep problems have other drivers (cortisol dysregulation, anxiety, sleep apnea), those won't resolve with estradiol alone. For more on the hormone-sleep relationship, how hormones affect your sleep covers the full picture.
Mood may start to stabilize during weeks 2–4, though this is highly individual. Estrogen has direct effects on serotonin, dopamine, and norepinephrine, and declining estrogen during perimenopause is a genuine driver of mood instability. Women who experience significant mood swings, irritability, or low mood as their primary symptom often report this improving earlier than they expected. Women with clinical depression or anxiety as a primary concern may need additional support beyond HRT.
Weeks 4–6: Sleep and Energy Shift More Clearly
By weeks four to six, you should be noticing more consistent improvement in sleep quality, not just on the nights when hot flashes happen to be mild, but as a sustained pattern.
Energy and fatigue often begin to lift in this window. Perimenopause fatigue has multiple drivers, poor sleep, declining estrogen's effect on mitochondrial function, and often subclinical thyroid issues running concurrently, so HRT addresses some but not necessarily all of them. If fatigue is persistent past this window despite improving sleep, it's worth checking thyroid function separately.
Progesterone side effects, if you're taking combined HRT (estrogen plus a progestogen), may be most prominent in this window. Oral micronized progesterone can cause drowsiness, bloating, or low mood in some women, particularly in the first few weeks. Many women find that taking progesterone at night mitigates the drowsiness and can actually improve sleep quality. If you're experiencing pronounced side effects from progesterone, discuss them with your provider, the form and timing of progestogen can be adjusted.
Weeks 6–8: Mood, Brain Fog, and Concentration
This is the window where cognitive and mood-related changes tend to become more apparent, and where women who've been waiting for the "mental" symptoms to resolve often start feeling the shift.
Brain fog and concentration respond more slowly to HRT than vasomotor symptoms. Estrogen supports synaptic function, cerebral blood flow, and neuroinflammatory regulation, and these processes take longer to recalibrate than the thermoregulatory effects. By weeks 6–8, many women begin noticing that word retrieval is easier, that they can hold a thought longer, or that the mental haziness that characterized their worst days is lifting.
The link between perimenopause and brain fog is well-established biologically, and the good news from recent research is that cognitive symptoms related to estrogen decline appear to be substantially reversible with timely estrogen replacement.
Mood stabilization should be more established by this point. If you're still experiencing significant mood swings, anxiety, or low mood at week 6–8, it's worth evaluating whether your dose is adequate. A dose that's too low won't fully stabilize estrogen's neurotransmitter effects, and symptoms will persist. The signs that your HRT dose may need adjusting are worth reviewing at this point in your journey.
Weeks 8–12: Genitourinary Symptoms, Skin, and Joints
Symptoms that depend on tissue-level changes take the longest to respond, and this is the window where they typically begin to show meaningful improvement.
Vaginal dryness and genitourinary symptoms, including discomfort with intercourse, urinary urgency, and recurrent UTIs, are driven by the thinning and loss of elasticity in urogenital tissue that estrogen normally maintains. Restoring estrogen levels begins reversing this, but tissue remodeling takes time. Most women see meaningful improvement in vaginal symptoms between weeks 8–12, with full benefit sometimes taking 3–6 months, particularly if tissue atrophy was significant. Vaginal dryness during perimenopause covers treatment approaches including local estrogen for women who need additional genitourinary support.
Joint pain is one of the more underappreciated symptoms of estrogen decline. Estrogen has anti-inflammatory effects on joint tissue, and perimenopause joint pain is reported by the majority of women in the menopausal transition. Many women notice significant improvement in joint stiffness and aching by the 8–12 week mark, though this varies with baseline inflammation.
Skin changes, dryness, loss of elasticity, increased sensitivity, also respond in this window. Collagen production, which estrogen supports significantly, begins recovering, though visible skin changes take longer than symptomatic ones.
Month 3 and Beyond: The Bigger Picture
By month three, you should have a reasonably clear signal about whether your current regimen is working for you. Hot flashes should be substantially reduced. Sleep should be consistently better. Mood and cognition should have improved meaningfully.
If you've reached month three and symptoms are only partially improved or have returned after early relief, it's not a sign that HRT has "stopped working", it's a sign that something in the regimen needs evaluation. The most common reasons include:
- Dose is too low for your absorption or your symptom burden
- Form isn't absorbing adequately, particularly relevant with certain topical preparations
- Other hormones are contributing, thyroid, cortisol, and testosterone all interact with how you feel on estrogen
- Life circumstances have shifted, stress, sleep disruption, and illness all affect how HRT performs
Why your HRT stopped working is a detailed guide to troubleshooting each of these scenarios, and it's worth reading before concluding that HRT isn't the right path for you.
A Note on Monitoring: Don't Guess, Measure
The timeline above reflects what typically happens when estradiol levels are actually in a therapeutic range. But one of the most common reasons women don't progress through this timeline on schedule is that their dose isn't delivering adequate blood levels, and without tracking, there's no way to know.
A single lab test weeks after starting HRT captures your level at one moment. But as explored in why your hormones look normal but you still feel terrible, a snapshot can miss the patterns that explain persistent symptoms. Continuous or regular monitoring gives a clearer picture of whether your estradiol is consistently in range, or dipping in ways that explain the gaps in your symptom relief.
If you're tracking your response and want to understand what your numbers should look like at each stage, the first 90 days of HRT: what your hormones should look like is the companion piece to this guide.
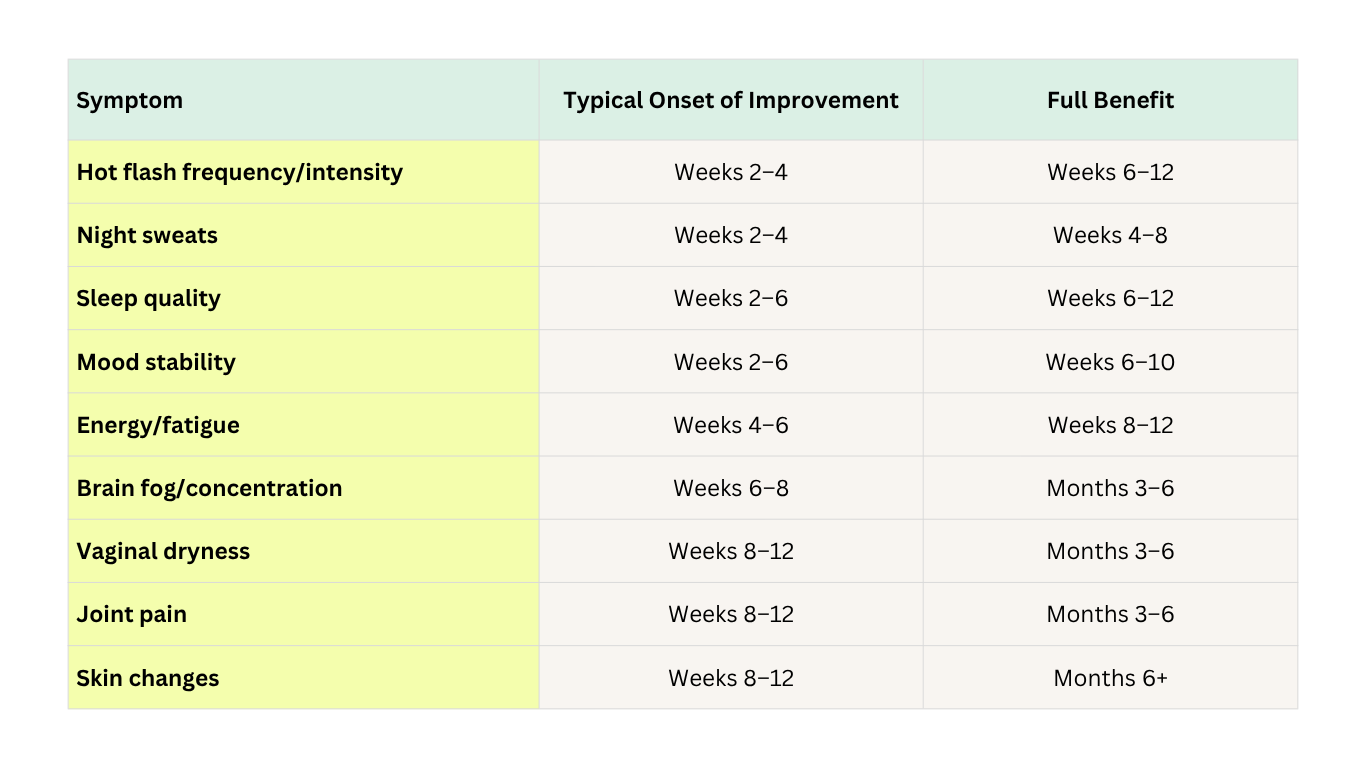
Quick Reference: HRT Symptom Timeline
The Bottom Line
HRT doesn't work on a single timeline, it works on multiple timelines simultaneously, with each symptom driven by a different biological mechanism. Hot flashes respond in weeks. Brain fog responds in months. Tissue-level changes take longer still.
Knowing this matters because the most common reason women stop HRT prematurely is expecting uniform improvement that doesn't come, and interpreting partial improvement as failure. It isn't. It's the expected pattern of a body recalibrating after years of fluctuating, then declining, hormone levels.
Give each symptom its window. Track your levels. Adjust the dose if the timeline is significantly off. And if something feels wrong rather than just slow, that's always worth a conversation with your provider, not a reason to stop.
About the author
Sources
- MacLennan AH, Broadbent JL, Lester S, Moore V. Oral oestrogen and combined oestrogen/progestogen therapy versus placebo for hot flushes. Cochrane Database Syst Rev. 2004;(4):CD002978. doi:10.1002/14651858.CD002978.pub2
- Santoro N, Epperson CN, Mathews SB. Menopausal symptoms and their management. Endocrinol Metab Clin North Am. 2015;44(3):497-515. doi:10.1016/j.ecl.2015.05.001
- Shifren JL, Gass ML; NAMS Recommendations for Clinical Care of Midlife Women Working Group. The North American Menopause Society recommendations for clinical care of midlife women. Menopause. 2014;21(10):1038-1062.
- Maki PM, Henderson VW. Hormone therapy, dementia, and cognition: the Women's Health Initiative 10 years on. Climacteric. 2012;15(3):256-262. doi:10.3109/13697137.2012.660613
- Sturdee DW, Panay N; International Menopause Society Writing Group. Recommendations for the management of postmenopausal vaginal atrophy. Climacteric. 2010;13(6):509-522. doi:10.3109/13697137.2010.522875
- The NAMS 2022 Hormone Therapy Position Statement Advisory Panel. The 2022 hormone therapy position statement of The Menopause Society. Menopause. 2022;29(7):767-794. doi:10.1097/GME.0000000000002028
- Prior JC. Progesterone for treatment of symptomatic menopausal women. Climacteric. 2018;21(4):358-365. doi:10.1080/13697137.2018.1472567
- Blumel JE, Castelo-Branco C, Binfa L, et al. Quality of life after the menopause: a population study. Maturitas. 2000;34(1):17-23.
- Lobo RA. Hormone-replacement therapy: current thinking. Nat Rev Endocrinol. 2017;13(4):220-231. doi:10.1038/nrendo.2016.164
- Genazzani AR, Monteleone P, Giannini A, Simoncini T. Hormone therapy in the postmenopausal years: considering benefits and risks in clinical practice. Hum Reprod Update. 2021;27(6):1115-1150. doi:10.1093/humupd/dmab026
About the Oova Blog:
Our content is developed with a commitment to high editorial standards and reliability. We prioritize referencing reputable sources and sharing where our insights come from. The Oova Blog is intended for informational purposes only and is never a substitute for professional medical advice. Always consult a healthcare provider before making any health decisions.



